Plantar warts
Discreet care, a clear plan, and a focus on effectiveness — without “shock imagery”. The goal is resolution, lower recurrence, and comfortable walking.
Note: as a rule, we do not request or receive clinical photos via WhatsApp. Use WhatsApp for booking and logistics.

Diagnosis
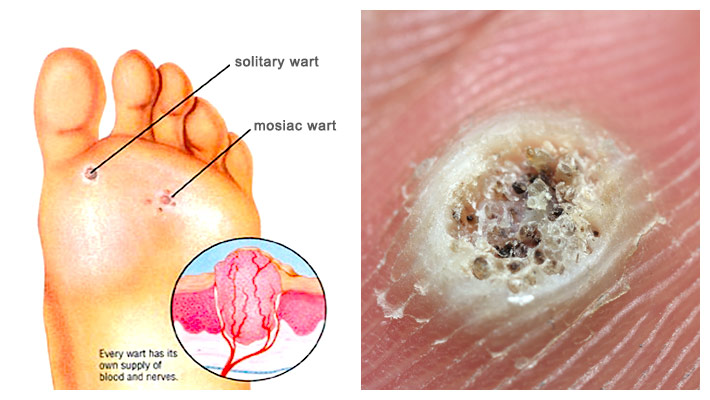
Visual check: “Is it a wart or a callus?”
The aim here is simple: help you recognise useful signs (without claiming a remote diagnosis). Confirmation is clinical.
- Interruption of skin lines.
- “Black dots” (thrombosed capillaries) may be present.
- Pain more on “side-to-side pressure” in some cases.
- Prolonged self-treatment without a plan.
- Repeated “burning” without a recurrence strategy.
- Ignoring hygiene/footwear and reinfection.
Important: not all cases show visible “black dots”. And not all plantar pain is a wart.
Treatments
Treatment choice should consider: location, pain, thickness, duration, recurrence risk, and patient tolerance. “One-size-fits-all” is usually the reason for failure.
Topicals (when appropriate)
- Technique matters: protect healthy skin and ensure adherence.
- Scheduled reassessment (not months of trial-and-error).
- Goal: reduce viral/keratin load and control symptoms.
Procedures
- Debridement/control of associated hyperkeratosis.
- Case-specific options (e.g., controlled destruction/ablation/energy).
- Follow-up plan to reduce recurrence.
Immunity + context
- Review persistence factors (humidity, changing rooms, footwear).
- Patient education: reinfection and “household transmission”.
- Combined plans often win resistant cases.
If you want, you can add a “Laser/energy” section here with your equipment and protocol, without graphic images.
Prevention
Survival kit (changing rooms, gym, pool)
Flip-flops always
In showers and shared wet areas.
Dry thoroughly
Between toes and plantar area (moisture = persistence).
Appropriate socks
Good breathability; change if you sweat.
Do not share
Files/pumice stones/household tools.
